The Centers for Medicare & Medicaid Services (CMS) issued an update to the State Operations Manual (SOM) on April 3, 2026, that introduces a significant shift in how surveyors evaluate and enforce requirements for patient discharges from skilled nursing facilities. The SOM, which guides state survey agencies in conducting compliance audits and determining enforcement actions, now includes new guidance on survey procedures that elevates certain discharge situations to a higher level of scrutiny.
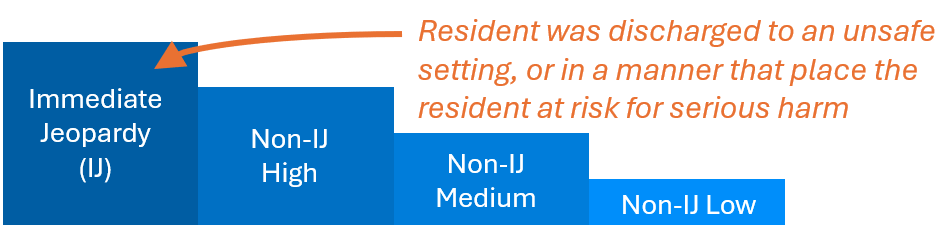
Specifically, the update adds language identifying intake scenarios that should be assigned an Immediate Jeopardy (IJ) priority, including cases in which a resident is discharged to an unsafe setting or in a manner that places them at risk of serious harm. The addition specifies:
“For nursing homes, all intakes where a resident was discharged to an unsafe setting, or in a manner that places the resident at risk for serious harm (e.g., the resident still has medical needs but they cannot be supported in the setting to which they were discharged).”
A Policy Shift Elevating Unsafe Discharges to Immediate Jeopardy Review
Citations related to unsafe discharges that place residents at risk are not new to the SOM. The manual already includes F tags that address this area, including F627 for inappropriate transfers and discharges that occur for reasons outside allowable criteria, and F628 for failures to provide proper notice or follow required discharge processes.
However, this update represents a meaningful escalation. For the first time, unsafe discharges are explicitly defined as an intake category tied directly to survey prioritization and Immediate Jeopardy review.
What This Means for Post-Discharge Documentation
This revised language builds on an ongoing shift in CMS policy, reinforcing that a patient’s success after discharge remains part of the facility’s continuing responsibility. As a result, providers are expected to demonstrate not only that a discharge was appropriate at the time it occurred, but also that the patient remained safe and supported afterward.
To meet this expanding expectation, providers must deliver effective post-discharge support, such as follow-up care, and maintain thorough documentation of these efforts to support compliance and defend against potential investigations or complaints.
For post-discharge follow-up calls, documentation should clearly demonstrate that the facility met its obligations to ensure a safe discharge. This requires more than a simple note that a call occurred. Records should include the date and time of the call, the staff member who initiated it, the individual contacted (whether the patient or a family member), and whether the patient or a family member.
In addition, documentation should reflect the substance of the follow-up, confirming key elements such as whether the patient received prescribed medications, remained clinically stable, and had appropriate support services in place, including home health, where applicable. Any concerns or grievances raised by the patient or family should also be thoroughly documented, along with timely actions taken to address them. This level of detail helps demonstrate a proactive approach and provides critical support in the event of survey review or complaint investigation.
As CMS continues to expand expectations around discharge accountability, facilities that treat post-discharge oversight as part of their core compliance strategy will be better positioned to mitigate risk.